Aug 14

Help Us Protect Access to Sexual and Reproductive Health Care Today!
On election night, I was so stressed I went to sleep at 10 pm; I just couldn’t handle watching the results. It felt like so much was at stake.
Now, weeks later, I am still trying to take in what it all means for our country, for the issues we care about – especially for access to comprehensive reproductive health care. One thing I know is that Congress will look very different in January. Women will make up 23.4% (125 members) of Congress – the highest number ever! And, we elected a very diverse group of women to Congress: Native American women from multiple states, multiple Muslim American women, Latinas from Texas and New York, the first African American women from Massachusetts and Connecticut.
A lot happened at the state level which will be critical for our work. The recent changes to the composition of the Supreme Court have left our right to access abortion more vulnerable than ever. States are taking steps to shore up their laws, one way or another, in anticipation of the erosion of Roe v Wade. Voters in Alabama, Oregon, and West Virginia weighed in on anti-abortion ballot measures. Oregon upheld the state’s abortion protections, but Alabama and West Virginia both passed legislation that will severely restrict access to abortion. With abortion access becoming more and more a state-based issue, it was heartening to see that many states elected pro-reproductive health officials to the governor’s houses and state legislatures.
I spent the days after the election at a planning retreat with my colleagues thinking about how our organization can best fulfill our mission in the years ahead. We charted an exciting, bold path which I will share in an upcoming newsletter. But, suffice it to say that we are focusing our energy and resources to make sure that everyone, everywhere has access to reproductive health care, especially abortion care.
As part of this work, the Reproductive Health Access Project is stepping up our efforts to protect access to reproductive health care. We are part of a coalition of 100+ reproductive health, rights, and justice organizations that outlined a proactive vision of sexual and reproductive health for our lawmakers. Our vision statement, A Call for Change, strongly asserts that “all people should have access to affordable, quality health care and as a part of that, access to health care providers that meet their needs, including their sexual and reproductive health needs.” We will be working in coalition with these organizations to ensure that our federal and state governments work to support this vision.
This work is hard and we are in this for the long haul. I am emboldened by the civic engagement demonstrated in the mid-term elections. People across the country care deeply about our issues and want to take action to make our country a better place. Together we can do it! Thank you for all you do to make this world a better place and for all you do for us! – Lisa Maldonado, MA, MPH, Executive Director
 At RHAP we believe everyone has the right to make the decisions that are best for their lives and bodies. This includes decisions about whether to have an abortion and what that abortion experience is like. One area that RHAP is paying close attention to is medication abortion, sometimes referred to as the “abortion pill.”
At RHAP we believe everyone has the right to make the decisions that are best for their lives and bodies. This includes decisions about whether to have an abortion and what that abortion experience is like. One area that RHAP is paying close attention to is medication abortion, sometimes referred to as the “abortion pill.”
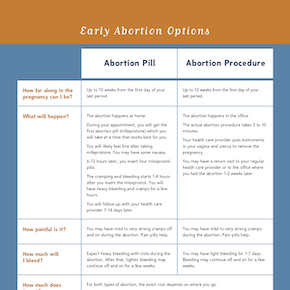
Medication is one of the options to end a pregnancy within the first 10 weeks. The most effective and most common medication abortion regime used in the United States consists of taking 5 pills: 1 mifepristone pill and 4 misoprostol pills. The mifepristone blocks the hormone progesterone, which stops the body from continuing to grow the pregnancy. The misoprostol, which is taken 6-72 hours after the mifepristone, causes the uterus to cramp and bleed, which helps the body to pass the pregnancy tissue. Patients looking to use this option may be able to obtain the medication from their clinician. Clinicians can dispense the mifepristone in their office and then write a prescription for misoprostol. The mifepristone pill is swallowed and the misoprostol pills can either be inserted into the vagina or placed in the mouth between your cheeks and gums where it will be absorbed by the body for 30 minutes. The misoprostol will cause cramping and heavy bleeding for 3-5 hours and may have side effects of nausea, diarrhea, and chills. Using medication to end a pregnancy is very safe, effective, can be used in the privacy of one’s home, and may feel more natural or discrete because the process is similar to what happens to the body with a miscarriage. In very rare cases, individuals using medication for an abortion may experience more serious symptoms that require reaching out to a clinician, including bleeding through more than two maxi pads per hour for two hours, not bleeding within 24 hours of taking the misoprostol pills, or feeling very ill after the heavy cramping and bleeding is over.
In places where mifepristone is not available, 4 misoprostol pills taken every 3-12 hours up to three times can also be used to end a pregnancy safely and effectively.
Medication abortion can be a good option for many people looking to end their pregnancies, particularly during this tumultuous time when abortion access is on the decline. For additional resources on medication abortion, check out RHAP’s Resources page.
From now until December 31st, RHAP is raising funds to train and support clinicians to provide comprehensive reproductive health care and to become outspoken reproductive health champions. With anti-abortion extremists working hard to deny us access to basic health care, reproductive health care is under constant threat. We count on supporters to help us do our work. Abortion Access is in YOUR Hands. Here’s how your donation helps expand and preserve access to reproductive health care:
$1,000 provides two full days of hands-on training in abortion.
$500 purchases one pelvic model for hands-on training in reproductive health care.
$250 covers the cost of training 20 clinicians to provide a medication abortion.
$90 provides a start-up supply of the pills needed for a medication abortion.
Thanks to two of our amazing supporters, donations will be matched dollar-for-dollar, up to $15,000, if you donate by December 31st.
You can also start a fundraiser for RHAP and use your network to spread the message and raise funds to support this important work today.
Every dollar counts! Whether it is $25, $50, or $150, your support today will make a difference towards access to reproductive health care.
If you have any access about our year-end campaign, Abortion Access is in YOUR Hands, please contact our Development Officer, Nushin Bhimani at nushin@reproductiveaccess.org.
As always, your support keeps us inspired!
 Just in time for the holiday season, Shelby Adler and Jay Louik started a fundraiser to benefit the Reproductive Health Access Project. “We’ve seen first-hand how RHAP empowers physicians to better counsel patients regarding their reproductive care.” Together, they raised a total of $445 for RHAP. We appreciate you, Shelby and Jay!
Just in time for the holiday season, Shelby Adler and Jay Louik started a fundraiser to benefit the Reproductive Health Access Project. “We’ve seen first-hand how RHAP empowers physicians to better counsel patients regarding their reproductive care.” Together, they raised a total of $445 for RHAP. We appreciate you, Shelby and Jay!
Would you also like to take action and support our work during this holiday season? If so, start your own fundraiser for RHAP today. We just launched our own tools so that you can have a DIY fundraiser to support us. Use your creativity and passion to take an active role by fundraising and spreading awareness for access to reproductive health care. If you’d like to start a fundraiser for RHAP, fundraise in your community, workplace, or in other ways, click here and start fundraising today!
 For this month’s Notes from the Field, we are sharing a patient experience from one of our Network members, Dr. E. Dr. E is a former RHAP fellow and member of the Mid-Atlantic Cluster who practices in the Delmarva area of Maryland, which is largely rural.
For this month’s Notes from the Field, we are sharing a patient experience from one of our Network members, Dr. E. Dr. E is a former RHAP fellow and member of the Mid-Atlantic Cluster who practices in the Delmarva area of Maryland, which is largely rural.
A few weeks ago, a 17-year-old female patient and her mother came to Dr. E for a follow-up visit for a medication abortion. The young woman was still experiencing bleeding and cramping three weeks after she took the abortion pills, and was becoming very anxious that the abortion “hadn’t worked.”
“She came to see me because the pain was so bad that she had missed school that day. She actually had to drive across state lines to New Jersey to get her medication abortion, so she wasn’t able to go back to that clinic – they told her to go to her primary care provider if she needed to have a follow-up appointment.” The nurse who checked the patient in came to Dr. E, worried that they wouldn’t be able to take care of her.
“Once I heard the situation, I told the nurse, ‘We got this! We’re okay!’ and the patient came in. She was very nervous, so we talked for a while before giving her a pregnancy test, which was negative. She got visibly calmer as I provided her reassurance that the abortion worked and that sometimes you can have some bleeding for a while. I offered her another dose of misoprostol to help decrease the bleeding, and then we talked about contraception. She told me she doesn’t want to get pregnant again, so we used the RHAP Birth Control Fact Sheet and went over every single method. She decided on the Depo Shot and I was able to prescribe it to her that day.”
For Dr. E, this experience further highlighted the importance of pushing for access to medication abortion in her clinical setting. “Because of where she lives, the closest in-state clinic was a Planned Parenthood, where she would have had to wait two weeks, making her ineligible for the medication abortion. Instead, she drove to another state, which speaks to the importance of having local providers who are available and able to offer these services right in our community.” As an added bonus, her patient was able to receive treatment in her primary care clinic, rather than in the Emergency Department (where many patients with bleeding tend to go).
Dr. E shared that this patient’s story reminded her of why she appreciates the training she received in the Fellowship, and how it’s helping her now as a family physician in a rural community health center. “When she presented, before I even spoke to her and I heard what was happening, I had a moment where I was like ‘Oh! I know what this is and I know how to manage it right now!'” The Reproductive Health Care and Advocacy Fellowship trained Dr. E to be able to offer patient-centered, full-spectrum reproductive health care as part of her family medicine practice. “They left with smiles on their faces, reassured that everything was okay… it was really rewarding and reminded me of why I do this type of care.”
Your gift allows us to train and support health care providers across the United States so they can offer patients compassionate and comprehensive care.
Aug 14